
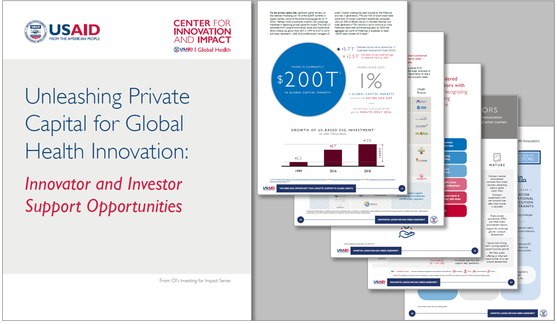
UNLEASHING PRIVATE CAPITAL FOR GLOBAL HEALTH INNOVATION
Innovator and Investor Support Opportunities
Join Global Health on Follow Global Health on
JUST LAUNCHED: UNLEASHING PRIVATE CAPITAL FOR GLOBAL HEALTH INNOVATION

The global community has committed to an ambitious set of 17 Sustainable Development Goals (SDGs) through 2030 – including SDG3 – “to ensure healthy lives and promote well-being for all at all ages.” Yet multiple recent estimates suggest that we are not on track to reach the health targets – even if we massively scale up coverage of existing interventions including medicines, vaccines, bed nets, and medical devices.
We will therefore need significantly more innovation – and funding to support that innovation – if we are to successfully achieve our global health aspirations. There is good reason to believe that both are possible – that we can encourage transformative innovation and that we can effectively mobilize more private capital to support those innovation efforts.
Unleashing Private Capital for Global Health Innovation takes stock of the needs of innovators and investors. This report:
- Lays out the challenges and opportunities of innovating and investing in global health
- Proposes a catalytic early stage “Innovator Support Facility” designed to increase the number of promising innovators successfully navigating the “valley of death” and reaching a point where they can attract and absorb more traditional sources of private capital
- Proposes a blended finance & global health “Investor Support Facility” designed to provide low cost risk capital to offset lower risk-adjusted returns in global health and ‘crowd-in’ a wider array of private investors
Building on this work, we will further explore, design, and test these solutions generated over the coming months to take these solutions forward. We encourage your feedback and partnership in this effort so that we can continue building, adapting, and turning innovation into impact.
Click the above link to view and download the report.

CRVS NOW OFFERED FREE TO LOW INCOME COUNTRIES TO MODERNIZE THEIR CRVS SYSTEMS
CRVS NOW OFFERED FREE TO LOW INCOME COUNTRIES TO MODERNIZE THEIR CRVS SYSTEMS https://www.crvsnow.com/
http://www.aihtsagamhub.com/s/getLinkedFile?filename=CRVSNOWPublicReleasMarch12019.pdf
Blog post- Building National Civil Registration Systems that Ensure Effective Service Delivery: http://blogs.worldbank.org/health/building-national-identification-systems-ensure-effective-service-delivery
Delivery of the state-of-the-art, comprehensive CRVS eLearning course: http://www.aihtsagamhub.com/s/getLinkedFile?filename=CRVS eLearning course info card.pdf
SYDNEY, AUSTRALIA – March 1, 2019 - CRVSNOW, the first commercially available cloud-based Civil Registration and Vital Statistics System with the largest installed base in the world, is being offered for free to low income countries. https://www.crvsnow.com/
Object Consulting recently implemented CRVS Solutions’ system, called CRVSNOW, in Victoria, Australia for 6.3M citizens. With this most recent success, CRVSNOW manages the life events for 14M citizens, handles 16,500 users, 123M vital records and prints 880,000 certificates a year. CRVSNOW is the most modern full-function commercially available cloud-based CRVS system in the world.
CRVS Solutions is now offering the latest release of CRVSNOW free to low income countries to support the modernization of their CRVS systems. CRVS Solutions’ offer includes a free test system and no mandatory support fees so interested countries can evaluate CRVSNOW online at no cost.
"Modern electronic systems that can link civil registration with civil identification system, particularly while assigning unique identification numbers to individuals at birth and with other information systems, can be a key factor in improving the access of these individuals to critical public services such as education, health, social welfare, and financial services,” said Dr. Samuel Mills who leads the implementation of the World Bank Group (WBG) 2016–2030 Civil Registration and Vital Statistics (CRVS) Action Plan".
Mills negotiated with CRVS Solutions to make CRVSNOW available to interested low-income countries for free. However, Mills emphasized that the WBG does not endorse specific vendor products; WBG encourages countries to assess several products to make informed decisions on the best overall value for money while considering quality, cost, and other factors as needed.
CRVSNOW has three main modules: 1) Core for staff and registry operations; 2) eRegistry – user interface and web service interfaces for hospitals, funeral directors, marriage celebrants and other stakeholders; and 3) ePublic – for all citizens to access the services of the registry e.g., parents registering the birth of a child. All modules are free for Low Income Countries.
Several countries are implementing a social registry for social safety net programs. A Social Registry is key to implementing social programs and enabling the delivery of successful outcomes consolidates the outreach, registration and assessment of needs and conditions of populations likely to be targeted by social programs. CRVSNOW is a platform to support any registry including a Social Registry.
“CRVSNOW is now proven in the two largest states of Australia with over 14M citizens. As part of our corporate social responsibility policy, we are very pleased to offer CRVSNOW to UN designated Low Income Countries for free to help them improve registration of vital events and contribute to furthering the UN’s SDG’s. Our team is experienced and ready to assist Low Income Countries to adopt CRVSNOW.” said Graham Jones, Group Business Development Manager for CRVS Solutions.
CRVSNOW can be customized to suit local context. The user interfaces for the system use RESTful APIs to communicate with the application servers. The user interfaces are written in Angular which is very flexible about formatting and style which allows a considerable degree of control, but CRVS Solutions can provide the source code for specific forms to allow countries to make their own version. Countries can integrate their own user interfaces into the API if desired.
CRVSNOW has an offline feature called the Field System. The Field System is a complete CRVSNOW system on a laptop. It is designed to be taken into the field where there are no network connections such as remote villages or islands. Because it is a complete system and it contains the registry (encrypted and with additional security), registry operations such as entering notifications, producing certificates and searching the registry can be conducted in the field with no Internet connection. Any notifications that are entered are saved in a “draft” list and then later submitted to the core when the Field System is reconnected to the network.
Jones added, “Whilst CRVSNOW was built for the high end needs of a high-income country, every country can use these features to improve data quality, make registration more accessible to every citizen and gain the cost benefits of cloud computing. Low income countries can start off using the core functions and then later use the high-end features without incurring any additional license costs.”
Further details, videos and downloads are available through the website at: https://www.crvsnow.com/
CRVSNOW is owned by CRVS Solutions Pty Ltd, a wholly owned subsidiary of Object Consulting Pty Ltd. CRVSNOW is a modern system which uses a range of best of breed open source products such as Tomcat, MongoDB, and Solr. The application servers are written in Java and the user interfaces in Angular. CRVSNOW integrates with external systems through APIs – RESTful and SOAP. It can receive data from external systems (normally as submissions) and can send data to external systems to update or inform them. There are also reporting and data export options specifically designed for sharing data to external agencies and organizations in a timely and automated manner (e.g., immigration, health, education, and statistics).
About CRVS Solutions Pty Ltd
CRVS Solutions is a wholly owned subsidiary of Object Consulting which is solely dedicated to the implementation of CRVSNOW in jurisdictions around the world.
About Object Consulting Pty Ltd: https://www.objectconsulting.com.au/
Object Consulting is Australia’s leading IT consultancy supporting organizations through their digital transformation journey. Driven by a strong focus on innovation and technology excellence, we design, integrate and build compelling experiences that connect enterprise and government organizations with consumers, citizens and staff. Object responsible for the recent highly successful go-live of CRVSNOW in Victoria, Australia.
WEST AFRICA'S EBOLA OUTBREAK COST $53 BILLION STUDY
West Africa's Ebola outbreak cost $53 billion – study
Reuters: By Tom Miles , 24 October 2018
An Ebola outbreak that ravaged Sierra Leone, Guinea and Liberia in 2014 cost economies an estimated $53 billion, according to a study in this month’s Journal of Infectious Diseases. The study aimed to combine the direct economic burden and the indirect social impact to generate a comprehensive cost of the outbreak, which was the worst in the world.The outbreak ran from 2013 to 2016 and killed at least 11,300 people, more than all other known Ebola outbreaks combined. The vast majority of cases were in Guinea, Liberia and Sierra Leone.
The report’s authors, Caroline Huber, Lyn Finelli and Warren Stevens, put the economic costs at $14 billion and said the human cost was even greater, based on the people affected and a dollar figure that reflects the value of each human life. The total is far higher than previous estimates. In October 2014, the World Bank said the Ebola epidemic could cost $32.6 billion by the end of 2015 in a worst case scenario, but by November 2014 it dialed back that forecast to $3-4 billion. In 2016 the World Bank estimate of economic loss was $2.8 billion.
The 2003 severe acute respiratory syndrome (SARS) cost an estimated $40 billion, while the 2015-2016 Zika virus outbreak in the Americas was estimated to have caused $20 billion in social costs, the new study said.
But a repeat of the 1918 influenza pandemic could cost an annual 700,000 lives and $490 billion, the authors said, citing research published in 2016.
The new Ebola study factored in the impact on healthworkers, long-term conditions suffered by 17,000 Ebola survivors, and costs of treatment, infection control, screening and deployment of personnel beyond West Africa.
The biggest cost not previously accounted for was deaths from other diseases, as Ebola tied up healthcare resources and hospital admissions fell dramatically, adding $18.8 billion to the total bill.
During the outbreak there were 10,623 additional deaths from HIV/AIDS, tuberculosis and malaria, with 3.5 million additional untreated malaria cases.
Measles caused 2,000-16,000 extra deaths as 1 million children missed being vaccinated for measles, and 600,000-700,000 missed other vaccines.
But the authors added that they had limited information on the cost of deploying international health staff and military personnel, and they were obliged to place a value on human life, a widely accepted economic measurement.
Although the “value of a statistical life” (VSL) in North America and Europe is estimated at $7 million-9 million, the authors said, they took a figure from the only study in a West African context, with a VSL of $577,000 in Sierra Leone.
ENCOURAGING SERVICE DELIVERY TO THE POOR : DOES MONEY TALK WHEN HEALTH WORKERS ARE PRO-POOR ?
Sheheryar Banuri, Damien de Walque, Philip Keefer, and Paul Jacob Robyn
World Bank Policy Research Working Paper 8666, December 2018
Do service providers respond to pecuniary incentives to serve the poor? Service delivery to the poor is complicated by the extra effort required to deliver services to them and the intrinsic incentives of service providers to exert this effort. Incentive schemes typically fail to account for these complications. A lab-in-the-field experiment with nearly 400 health workers in rural Burkina Faso provides strong evidence that the interaction of effort costs, ability, and intrinsic and extrinsic incentives significantly influences service delivery to the poor.
Health workers reviewed video vignettes of medical cases involving poor and non poor patients under a variety of bonus schemes. Bonuses to serve the poor have less impact on effort than bonuses to serve the non poor; health workers who receive equal bonuses to serve poor and non poor patients see fewer poor patients than workers who receive only a flat salary; and bonuses operate largely through their influence on the behavior of pro-poor workers. The paper also presents novel evidence on the selection effects of contract type: pro-poor workers prefer the flat salary contract to the variable salary contract.
Research on Human Development/ Development Research Group/ All Policy Research Working Papers
Research Newsletter: Subscribe | Archived Issues/ Research eAlerts: Subscribe
Twitter | Question?
research@worldbank.org
THE WORLD BANK AND GLOBAL FINANCING FACILITY SOCIAL HEALTH INSURANCE IN GFF COUNTRIES: OPPORTUNITIES AND PITFALLS
Opportunities and Pitfalls
Washington, November 11, 2018
The paperAbstract
Authors: Susan F. Martin, Rochelle Davis, Grace Benton and Zoya Waliany, March 2018
Thematic Working Groups/ Forced Migration and Development/ Regions/Middle East and North Africa
INTRODUCTION
1. This paper examines the experience with Social Health Insurance (SHI) and compulsory health schemes in selected countries to help inform the policy dialogue with governments. The purpose of this paper is to assesses country experience with SHI and identify lessons for countries where the Global Financing Facility (GFF) is active. The paper examines (i) the merits and demerits of SHI to finance health systems in LICs and MICs when compared with other coverage schemes, (ii) the likely challenges for a country that tries to move forward with SHI and (iii) potential solutions. The paper is not meant to be a guideline to advice governments on SHI; rather, it aims to build a common understanding about SHI to inform the health policy dialogue with governments.
2. Several lower-income countries are considering Social Health Insurance as a method to mobilize and pool additional resources for health. Most countries supported by the GFF (13 of 23) do not have SHI for their population (Annex Table 1). Instead they finance and provide automatic health coverage through the government health sector. However, an increasing number of low-income countries are interested in SHI. Madagascar’s national policy for universal health coverage from December 2015 aims to develop national health insurance that pools contributions from taxes, external donor grants, and other sources (Garchitorena 2017). In 2015, Burkina Faso passed a law for universal health insurance (assurance maladie universelle) that will fully subsidize coverage for the poor and partially for low-income groups (Wright 2016). In Cameroun, the government is considering universal coverage to be financed from contributions paid by employers, employees and retirees, as well as the informal sector population1. Myanmar plans to develop a new social health insurance law2. These countries strive to provide health coverage for the entire population through national health insurance.
OUR HEALTH SYSTEMS AREN'T READY FOR THE RISING DEMAND FOR MENTAL HEALTH SERVICES
News;
https://www.intrahealth.org/vital/our-health-systems-aren%E2%80%99t-ready-rising-demand-mental-health-services
Photo by Nana Kofi Acquah for IntraHealth International.
"The mental health toll of obstetric fistula and other health-related traumas is great. The stomach-ache started soon after she gave birth to her last child, and it didn’t stop for years. When she finally made her way to a hospital, the doctors performed a hysterectomy—but it didn’t go well. A day later, she realized she was leaking urine. “I told them something wasn’t right,” the woman tells us. “But they told me everything was fine and that I needed to go home.”The woman says all this in a monotone as we sit under a tree outside the hospital.
The surgery had caused an obstetric fistula, which persisted over the next five years and forced her to go through several unsuccessful repair surgeries, until finally the last one—provided through IntraHealth International’s Fistula Mali project in May 2017—worked.
The woman says all this in a monotone as we sit together under a tree outside the hospital in Kayes, Mali, where her final surgery took place. Yes, we can take her picture, she says. But she doesn’t want us to show her face or use her name. Physically, she’s healed, but she doesn’t yet feel whole again. She still remembers the pain and isolation, the way family members covered their noses when she tried to visit them.
“People invite me over now, but I still refuse,” she says. “I’m in the habit of staying home and being alone now.”
A few months later, I was thinking about this woman as I sat in one meeting room after another at the 2018 Health Systems Research Symposium in Liverpool, UK. This is where thousands of experts come together every two years to discuss the latest findings in health systems and policy research and practice. There’s a lot to talk about, of course—HIV care, health services for young people, financing mechanisms, the eternal puzzle of community health worker programs.
Only a handful of times did the subject of mental health crop up in the program. But in the field of global health and development, our inattention to mental health is a huge problem, and it’s only getting bigger.
THE GREAT AND RISING NEED
In India, mental health is the second-leading cause of disability. Kaaren Mathias of the Emmanuel Hospital Association told us this during a session on strengthening mental health services. In the Indian state of Uttarakhand, she said, there are seven government-employed psychiatrists for 10 million people. Compare this to Sweden, for example, where there are 2,320 psychiatrists per 10 million people. India is one of many countries where mentally ill people are sometimes chained up by their necks, ankles, or wrists by family members and caretakers who don’t know how to care for them.
This happens in Timor Leste, too, Teresa Hall of the University of Melbourne told us. There is one psychiatrist for the entire country and families bear the burden of care.
Globally, 79% of suicides occur in low- and middle-income countries.
And in Ghana, where the treatment gap for mental health stands at 98%—meaning that only two out of every hundred people who need professional care can get it—unregulated traditional mental health centers step in to fill the gap. These are prayer camps, fetish priests, herbalists, and mystical and hypnotic practitioners, said Gina Teddy of the Ghana Institute of Management and Public Administration.
Many Ghanaians trust them over the formal health system, but because the centers are unregulated, they’re not held accountable for, say, overcrowding, imposing involuntary treatment, denying clients food or shelter or health care, or even chaining them up.
All of these examples are anecdotal, of course. But they’re all part of some troubling global numbers:
• Worldwide, one in five adolescents experiences mental health challenges. Most are underdiagnosed and undertreated.
• Over 21% of births worldwide involve adolescent mothers under the age of 19, and every year, 18.5 million girls give birth in poor regions. Perinatal depression is more common and has greater consequences for adolescent mothers—it’s associated with higher risks for poverty, poor physical health, poor fetal growth, parenting difficulties, and more.
• Among young people 15–29 years old, suicide is the second-leading cause of death.
• Globally, 79% of suicides occur in low- and middle-income countries.
• The global median number of mental health workers is 9 per 100,000 population, according to the World Health Organization’s Mental Health Atlas 2017—though clearly the variations from low- to high-income countries are extreme.
These numbers make it clear that we are not prepared. Even when it comes to meeting today’s mental health needs, our health systems fall far short. And for those who are displaced or war-weary or recovering from health-related traumas such as obstetric fistula or Ebola, the need is growing by the hour.
Plus, 42% of our worldwide population is under 25. Almost half live in South Asia and sub-Saharan Africa. The sheer volume of wide-ranging needs on the horizon will quickly overwhelm our existing mental health systems and professionals.
During her most despairing moments of living with obstetric fistula, she’d considered suicide, even attempted it.
There’s no easy solution. But by integrating mental health services into primary care and general health services at the community level, countries can start reaching more people in need. This is the strategy WHO is encouraging member states to adopt.
In Mali, I spoke with more than one woman who told me that during her most despairing moments of living with obstetric fistula, she’d considered suicide, even attempted it. So many said that before their repair surgeries, they felt abandoned, neglected, hopeless.
We can’t continue to under investigate and under invest in global mental health and well-being. If we go on neglecting this in our health systems, our health systems will go on neglecting far too many of us.
AFRICA CENTERS FOR DISEASE CONTROL AND PREVENTION
Africa Centres for Disease Control and Prevention - One year later
Vision
To strengthen Africa’s public health institutions’ capacities, capabilities and partnerships to detect and respond quickly and effectively to disease threats and outbreaks based on science, policy, and data-driven interventions and programmes
Mission
A safer, healthier, integrated and prosperous Africa, in which Member States can efficiently prevent disease transmission, implement surveillance and detection, and always be prepared to respond effectively to health threats and outbreaks
Africa Centres for Disease Control and Prevention (Africa CDC) to ensure Africans have a public health institution capable of mitigating against the social, economic, and security dimensions of infectious disease threats. Second, in July 2017, these leaders issued a declaration to accelerate the implementation of International Health Regulations (IHR) on the African continent.
Annual Report
As outlined in this annual report, considerable progress has been made in establishing the Africa CDC since it was launched in January 2017. The Africa CDC has primarily focused its operational activities on five strategic pillars: 1) surveillance and disease intelligence, 2) emergency preparedness and response (with a focus on pandemics), 3) laboratory systems and networks, 4) innovative information systems, and 5) public health institutes and research. From an administrative perspective, the Africa CDC governance structure and a corresponding policy manual have been developed and approved by the Africa CDC Governing Board. Recruitment of the first cohort of permanent staff is ongoing. Moreover, despite being in its infancy, Africa CDC effectively supported nine outbreak responses in several Member States during 2017.
In 2018, Africa CDC’s priorities include:
1.Support Member States to establish or strengthen National Public Health Institutes and the five Africa CDC Regional Collaborating Centres in Egypt, Nigeria, Gabon, Zambia, and Kenya.
2.Establish the Regional Integrated Surveillance and Laboratory Network (RISLNET) to ensure that all public health assets are efficiently
Establishing the Africa Centres for Disease Control and Prevention: One Year Later
Message from the Director: Dr. John Nkengasong
Africa bears the highest burden of infectious disease pathogens in the world but has the weakest public health systems and infrastructure. This situation poses a severe security and economic threat to the continent. For instance, the Ebola virus disease outbreak in West Africa killed an estimated 11,000 people and reversed fragile economic gains in the affected countries. More recently, the world has observed the emergence and re-emergence of infectious diseases with pandemic potential. Social and environmental determinants related to urbanisation, as well as increases in population size and mobility have created conditions conducive to the spread of infectious diseases. The population of Africa is expected to increase from 1.2 billion to 2.4 billion people by the year 2050. Additionally, the widespread use of medications has created an enormous threat due to emerging antimicrobial resistance.
To address these challenges, African leaders have taken two significant actions: first, in January 2017, African Heads of State and Government launched the Africa Centres for Disease Control and Prevention (Africa CDC) to ensure Africans have a public health institution capable of mitigating against the social, economic, and security dimensions of infectious disease threats. Second, in July 2017, these leaders issued a declaration to accelerate the implementation of International Health Regulations (IHR) on the African continent.
Recruitment of the first cohort of permanent staff is ongoing. Moreover, despite being in its infancy, Africa CDC effectively supported nine outbreak responses in several Member States during 2017.
In 2018, Africa CDC’s priorities include:
1.Support Member States to establish or strengthen National Public Health Institutes and the five Africa CDC Regional Collaborating Centres in Egypt, Nigeria, Gabon, Zambia, and Kenya.
2.Establish the Regional Integrated Surveillance and Laboratory Network (RISLNET) to ensure that all public health assets are efficiently
3.Establish a broad public health workforce agenda in the areas of the field epidemiology, laboratory leadership, and public health informatics. Africa CDC will also launch several public health leadership and Masters in public health scholar programmes.
4.Launch a public-private philanthropic partnership, given the economic threat that outbreaks and other public health emergencies pose to businesses, ensure that donors and technical partners closely coordinate their efforts with Member States, Africa CDC, and the World Health Organisation to ensure unified engagement.http://www.aihtsagamhub.com/s/getLinkedFile?filename=2017 Africa CDC Annual Report.dat
Lastly, Africa CDC expresses its gratitude to the partners that have stood with us since the inception of this exciting endeavour. Sincere thanks go to the following partners: The United States Government through the Department of Health and Human Services and United States Centres for Disease Control and Prevention and United States Agency for International Development, the Chinese Government through the China Centres for Disease Control and Prevention, the Japanese Government, the Kuwait Government, the World Health Organisation Regional Office for Africa and for the Eastern Mediterranean Region, the Bill & Melinda Gates Foundation, the Centres for Global Health Diplomacy in Washington DC, McKinsey and Consulting, UNAIDS (Joint United Nations Programme on HIV/AIDS), the International Association of National Public Health Institutes, and Emory University.
SURVIVE AND THRIVE: TRANSFORMING CARE FOR EVERY SMALL AND SICK NEWBORN
SURVIVE AND THRIVE: TRANSFORMING CARE FOR EVERY SMALL AND SICK NEWBORN -FOREWORD
http://www.aihtsagamhub.com/s/getLinkedFile?filename=WHO-FWC-MCA-18.11-eng.pdf
The launch of Every Newborn: an action plan to end preventable deaths at the Sixty-seventh World Health Assembly in 2014 (1, 2) coincided with a period of great progress. The global neonatal mortality rate declined from 31 to 18 deaths per 1000 live births between 2000 and 2017. But three years into the era of the SDGs, we are still far from our goal of reducing newborn deaths to 12 per 1000, or less, by 2030 in all countries.
Bending the curve further will require a laser-sharp focus on reorganizing health systems to provide quality care, and continuity of care, for newborns – especially those who are critically ill. To that end, every pregnant woman and every newborn, without exception, must have access to high-quality, affordable services before, during and after the time of birth. Accessible services are especially important for populations that are underserved and marginalized, including those living in humanitarian settings or in conflict. We also need more comprehensive “specialized and intensive” newborn care services – because services that are good enough for healthy newborns might not suffice for those who come into the world unwell.
This report is a much-needed wake-up call for investing in quality inpatient neonatal care and designating facilities for specialized and intensive newborn care. Simultaneous investments are required to ensure adequate and appropriate human resources, supplies, and laboratories and data systems for well-functioning, family-centred, inpatient neonatal care. The care provided during hospitalization and follow-up in the community also needs to be nurturing to promote the optimal physical and mental development of the child. Supporting healthy brain development during early childhood is the best investment a country and society can make in the future generation – and in continued economic growth.
We are proud that our respective organizations, along with numerous contributors and partners, are part of the joint effort that has reached these conclusions. Our collaboration has already yielded important results. With this report, we call upon governments, health
professionals, parents and other partners to join us in supporting continued investment in health systems that respond to the needs of the most vulnerable. In this way, we can – and we will – achieve the vision of a better world for every mother and newborn.
After all, newborns are not just bundles of joy for their families. They are a promise to the future.
INTERNATIONAL RESPONSIBILITY-SHARING FOR REFUGEES
International Responsibility-Sharing for Refugees
Abstract
Authors: Susan F. Martin, Rochelle Davis, Grace Benton and Zoya Waliany, March 2018
Thematic Working Groups/ Forced Migration and Development/ Regions/Middle East and North Africa
Responsibility-sharing is a core tenet of international responses to refugee crises. Too often, however, there are massive failures in responding collectively and cooperatively to large-scale movements of refugees and displaced persons. Responsibility-sharing is essential largely because the costs associated with protecting and assisting refugees and displaced persons are unequally placed. Where refugees go is often an accident of geography, with low- and middle-income states that are close to countries in conflict often called upon to host far larger numbers of refugees than wealthier, more distant states. The Global Compact on Refugees is expected to include a framework to enhance responsibility-sharing.
This paper argues for a holistic approach to responsibility-sharing that enhances the protection of refugees as well as policy responses that address the needs of host communities. It focuses on several areas of responsibility-sharing, including efforts to address the underlying causes of displacement within and across borders; efforts to find solutions, including resettlement of refugees from host countries to third countries; initiatives to enhance protection; financial support for refugees, internally displaced persons, and the communities in which they reside; and technical assistance and training for host countries and local organizations.
The paper examines these issues from the perspective of host country governments, other host country stakeholders, donor governments, service providers, and, most importantly, the refugees and internally displaced persons themselves. The paper includes a case study of attitudes toward responsibility-sharing among these actors in the Middle East and North Africa, where millions of refugees and internally displaced persons are located. The paper concludes with recommendations to enhance responsibility-sharing as well as mechanisms to alleviate the costs to host communities and broaden the benefits to refugees and hosts alike.
KNOMAD WP_International Responsbility-Sharing for Refugees.pdf